




Chiba Medical J. 101E:49-55, 2025
doi:10.20776/S03035476-101E-3-P49
〔 Case Report 〕
Nao Watanabe1), Kyoko Aoyagi1), Shigeki Nakano2)
Yoshinori Higuchi2), and Masayuki Ota3)
1) Gamma Knife House, Chiba Cerebral and Cardiovascular Center, Ichihara 290-0512.
2) Department of Neurological Surgery, Chiba University Graduate School of Medicine, Chiba 260-8670.
3) Department of Diagnostic Pathology, Chiba University Graduate School of Medicine, Chiba 260-8670.
(Received February 3, 2025, Accepted March 3, 2025, Published September 10, 2025.)
【Background】Vestibular schwannoma (VS) is a benign tumor, and gamma knife radiosurgery (GKS) is a treatment option for small and medium-size tumors. Radiation-induced cavernous malformation (RICM) , a rare type of radiation therapy injury, is predominantly reported in pediatric brain tumor cases. We report a rare case of rapid RICM formation more than 5 years post-GKS for VS, requiring surgical treatment.
【Observations】A 73-year-old man presented with left-sided hearing loss and was diagnosed with VS, for which he underwent GKS. Follow-up magnetic resonance imaging (MRI) showed a transient tumor expansion, followed by shrinkage. However, 5 years post-GKS, the patient developed worsening left hearing loss and ataxic gait. MRI revealed a 30-mm cystic lesion in the left cerebellopontine angle, exerting brainstem compression. The lesion was surgically excised, and histopathological analysis revealed features of both VS and cavernous malformation-like lesion.
【Lessons】This case highlights the occurrence of RICM 5 years after GKS for VS, leading to rapid neurological decline. Although exceedingly rare, long-term follow-up should be considered to avoid rapid deterioration of neurological symptoms due to RICM. Surgical excision is recommended for symptomatic lesion and provides symptomatic relief.
Gamma knife radiosurgery (GKS), Vestibular schwannoma, Radiation-induced cavernous malformation (RICM), Delayed cyst formation, Case report
Vestibular schwannoma (VS) is a benign tumor, with treatment options including surgical resection, radiation therapy, or observation, depending on tumor size, hearing status, and patient preference. Gamma knife radiosurgery (GKS) is indicated for tumors less than 3 cm in diameter, with effective tumor control reported by numerous studies [1-5]. GKS is minimally invasive, making it particularly suitable for elderly patients or those at high surgical risk due to poor general health. It may also preserve hearing function[4,6].
However, various radiation-induced adverse events can occur following radiation therapy for brain tumors [7]. Radiation-induced cavernous malformation (RICM) is such a type of radiation injury, most commonly found in the supratentorial deep white matter after treatment of childhood medulloblastomas and gliomas[8,9]. To date, only two cases of RICM following radiotherapy for VS have been reported[7,10]. We report a very rare case of rapid RICM formation approximately 5 years post-GKS for VS, necessitating surgical intervention.
A 73-year-old man presented with left-sided sudden sensorineural hearing loss in 2015 (Fig. 1, timeline figure). The patient underwent magnetic resonance imaging (MRI), which revealed a mass lesion with a maximum diameter of 20 mm in the left cerebellopontine angle (CPA) (Fig. 2A). The patient was diagnosed with Koos grade 3 vestibular schwannoma and underwent GKS in 2016. The prescribed peripheral dose was 12 Gray (Gy) at a 53% isodose line, with a 96% coverage (Fig. 2B, C). The initial tumor volume was 3.260 cc. His hearing status was improved before GKS.
Follow-up MRI showed transient tumor volume expansion[11] to 4.220 cc at 3 months post treatment (Fig. 1, Fig. 3A), followed by shrinkage to 2.220 cc at 6 months (Fig. 3B). By 5 years post-GKS, the tumor volume had remarkably decreased, with a maximum diameter of 8 mm and a volume of 0.295 cc (Fig. 3C).
However, 5 years and 7 months after treatment, the patient developed worsening left-sided hearing disturbance and ataxic gait. MRI revealed a 30 mm cystic lesion in the left CPA, causing brainstem compression (Fig. 3D-F). The patient also experienced left trigeminal neuropathy, left abducens neuropathy, left facial nerve palsy, severe gait instability, and inability to walk.
The cystic lesion was surgically excised via craniotomy with a lateral suboccipital approach, removing over 95% of the lesion. A small remnant attached to the facial nerve and brainstem within the cerebral cistern was preserved. The cyst contained old hemorrhagic xanthochromic content and a nodule-like lesion resembling a cavernous malformation (Fig. 4A, B).
Histopathological analyses revealed spindle-shaped cells with elongated nuclei and eosinophilic endoplasmic reticulum. The lesion included hemorrhage, a hemosiderin-phagocytic histiocyte cluster, an inflammatory infiltrate of lymphocytes and plasma cells, and a spongiform vascular malformation-like structure with numerous small and large dilated thin-walled irregular muscular vessels (Fig. 4C, D). Immunostaining identified a mixture of alpha-smooth muscle actin (α-SMA) -positive and α-SMA negative vessel walls within the cavernous malformation-like component, suggesting partial α-SMA antigenicity reduction due to preoperative treatment-induced degeneration. The histology of the vessels was different from that of typical cavernous malformations, with predominantly thinned vessel walls lacking commensurable smooth muscle. In addition, spindle-shaped tumor cells, positive for S100 and SRY-Box Transcription Factor 10 (SOX10), were intercalated among these vessels. The pathological diagnosis was a mixture of vestibular schwannoma and a cavernous malformation-like lesion.
Postoperatively, the patient’s ataxia and cranial nerve disturbances improved measurably (Fig. 4E).
Fig. 1 Timeline of symptoms, treatment and tumor volume. SSNHL, sudden sensorineural hearing loss; GKS, Gamma knife surgery
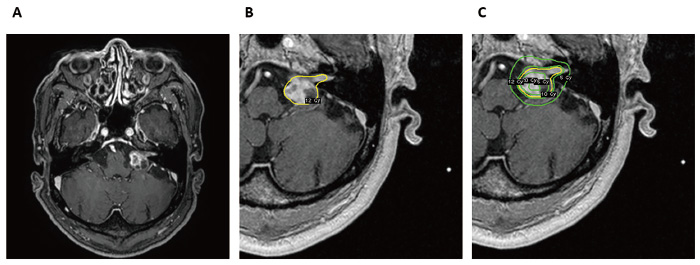
Fig. 2 A: Initial axial T1-weighted post-contrast MRI showing a left vestibular schwannoma with tumor volume of 3.260 cc. B, C: The tumor was treated with GKS with a prescribed peripheral dose of 12 Gray (Gy), 53% isodose line, and covering 96%. The yellow line indicates the 12 Gy isodose curve and the green lines indicate the 5 Gy, 10 Gy and 15 Gy from the outside to the inside, respectively.
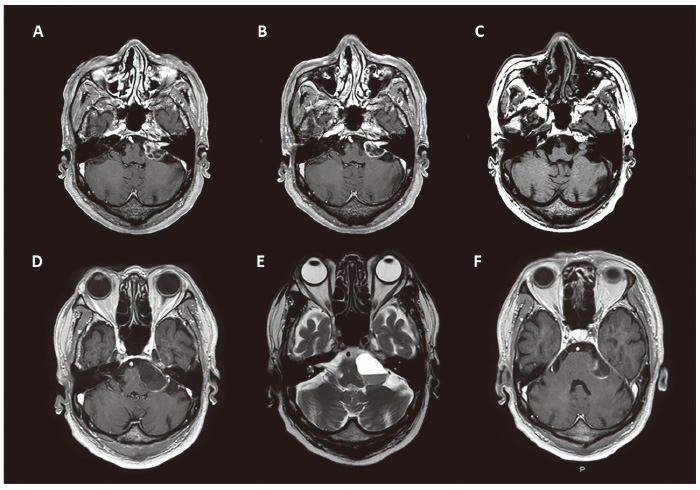
Fig. 3 A: Follow-up image at 3 months after GKS showing transient expansion (tumor volume 4.220 cc). B: Tumor volume showed a decrease from the initial volume of 2.220 cc at 6 months after GKS. C: The tumor volume remarkably decreased to 0.295 cc at 5 years after GKS. D-F: 5 years and 7 months after treatment, the patient developed worsening left hearing loss and ataxic gait, and MRI revealed a large cystic lesion (tumor diameter, 30 mm) with an internal nodule in the left CPA, presenting compression of the brainstem. D, F: axial T1-weighted post-contrast MRI, E: axial T2-weighted MRI.
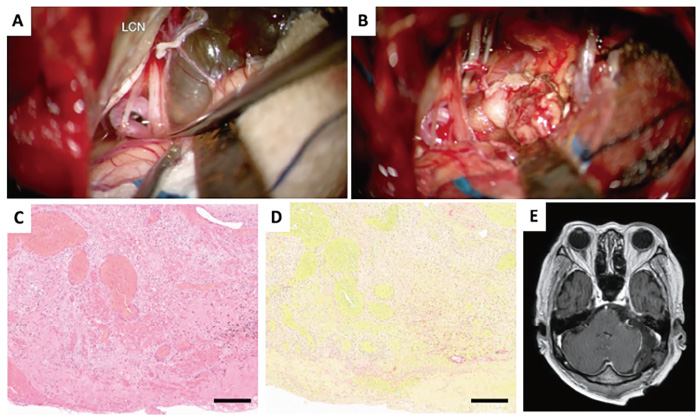
Fig. 4 A: Microscopic image of tumor removal. The cystic lesion was attached to the facial nerve and brainstem in the cerebral cistern. B: Inside the cyst, there was an old hemorrhagic xanthochromic content and a nodule-like lesion resembling a cavernous malformation. C: Original magnification is ×200. Hematoxylin and eosin stain illustrating a mixture of VS and cavernous malformation-like histology, which contains a spindle-shaped cell population consisting of elongated nuclei and eosinophilic endoplasmic reticulum, with a hemorrhage and hemosiderin-phagocytic histiocyte cluster, an inflammatory cell infiltrate consisting mainly of lymphocytes and plasma cells, and a spongiform vascular malformation-like component with numerous small and large dilated thin-walled, irregular muscular vessels. D: Elastica van Gieson stain demonstrated lack of elastic fibers surrounding the vessels. E: More than 95% of the cystic lesion was removed, and ataxia and cranial nerve disturbances improved. Black bar = 250 μm.
Transient increases in tumor volume are commonly observed after GKS for VS, usually within six months after irradiation, followed by shrinkage. The present case of rapid tumor growth after a prolonged period of tumor shrinkage (five years) is rare, suggesting a mechanism distinct from that of transient expansion or tumor recurrence.
GKS for VS has demonstrated good long-term tumor control; Hasegawa et al. reported good local control rates of 93%, 91%, and 89% at 5, 10, and 15 years, respectively, with peripheral doses below 14 Gy. For cases without brainstem compression or fourth ventricle deformity, GKS is a minimally invasive treatment associated with low rates of facial nerve palsy and high hearing preservation, particularly when performed early, compared to surgical treatment[2,3]. Transient expansion is a phenomenon observed after GKS for VS, which should be noted as it can sometimes become symptomatic and require surgical intervention [11]. Transient expansion can occur after GKS for VS, typically peaking between 6 and 9 months post-treatment, with tumor volumes increasing up to 1.5 times their initial size. Half of the tumors usually take an average of 12 months to shrink and return to their pre-treatment size, although about 10% remain larger than their pre-treatment size five years later. The causes of transient expansion are not fully understood but may involve radiation-induced tumor necrosis, chronic intratumoral hemorrhage due to delayed radiation injury, or biological responses to radiation[11]. In the present case, transient expansion was observed after 3 months of treatment, and then the tumor began to shrink and remained under control, which is expected, but unexpectedly rapid tumor growth with cyst formation was observed.
Delayed complications, including cyst formation, enlargement of preexisting or extratumoral cysts, and malignant transformation, remain possible causes of long-term treatment failure after GKS for VS[1]. Cyst formation is the most common long-term complication after GKS for cerebral arteriovenous malformations and metastatic brain tumors, and rarely reported after GKS for VS[12-15]. The pathological characteristics of this cyst formation are described as hemorrhage with dilated capillary vessels and wall thickening and degeneration, which differ from the pathological findings in the present case.
Adverse events due to radiation-induced brain injury have been documented. Complications include meningioma, glioma, cavernous malformation, enlarged perivascular space, leukoencephalopathy, stroke-like migraine after radiation therapy, moyamoya disease, radiation necrosis, endophthalmitis, optic neuropathy, and retinopathy[7]. In the present case, cavernous malformation-like pathology suggests RICM as the underlying cause.
RICMs are most commonly reported in pediatric cases, particularly following treatment for medulloblastomas and gliomas. There are two types of RICM: one that occurs in pediatric patients and another that is observed in adults. In one observational study, over 60% of RICMs occurred in the supratentorial deep white matter of the frontal and temporal lobes [16]. In adults, most patients often showed RICM in the irradiated area[9,16-18]. RICM has been reported to occur after GKS for astrocytoma, AVM, and epilepsy [19,20]. However, its occurrence after GKS for VS is especially rare and to date, only two reports of RICM after GKS for VS exist[7,10].
RICM is characterized by chronic minor hemorrhage due to vascular injury that then underwent revascularization, forming a cohesive mass mimicking cavernous malformation[15]. Edema, vasodilation, necrosis, and gliosis occur after irradiation, which may lead to the formation of a CM-like lesion[7,19,21]. Pathological features of RICM include thinned vessel walls with indistinct borders and lack of SMA immunoreactivity due to the absence of smooth muscle fibers, distinguishing them from non-radiation-induced CM[19,22]. The pathological findings in the present case revealed thin-walled, irregular muscular vessels, intervening schwannoma cells, and a lack of smooth muscle fibers in some vessel walls. Although not entirely consistent with typical RICM pathology, it was clearly different from typical CM pathology and suggests a delayed radiation-induced adverse event.
This case highlights the occurrence of RICM approximately 5 years after GKS for VS, followed by a rapid deterioration of neurological symptoms. The pathology of the present case was not fully compatible with CM; however, the hemorrhagic cyst formation after stereotactic radiosurgery for VS may be related to the adiation-induced histological change. Although extremely rare, this case underscores the importance of long-term follow-up to avoid transient deterioration of neurological symptoms and re-aggravation of the lesion due to RICM. Surgical excision is recommended for symptomatic lesion and provides symptomatic relief.
S. N. performed the surgical treatment. M. O. performed the pathological evaluation. N. W. wrote the manuscript under the supervision of K. A. and Y. H. All authors read and approved of the final manuscript.
The authors did not receive any Grant or funding source.
The authors have no conflicts of interest.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
All data generated or analyzed during this study are included in this published article.
Address correspondence to Dr. Kyoko Aoyagi.
Gamma Knife House, Chiba Cerebral and Cardiovascular Center,
575, Tsurumai, Ichihara 290-0512, Japan.
Phone: +81-436-88-3111.
E-mail: kyotsuru0108@gmail.com
